Introduction: A Common Condition Hidden in Plain Sight
Erectile dysfunction (ED) is not a rare or marginal condition. It is a highly prevalent, age-associated, vasculogenic and psychosocial disorder that affects quality of life as profoundly as many chronic systemic diseases. The definition is straightforward—persistent inability to achieve or maintain an erection sufficient for satisfactory sexual performance—but its implications extend far beyond penile hemodynamics. ED influences emotional health, partner relationships, self-esteem, and even healthcare engagement.
In Asia, ED represents a particularly complex medical and sociocultural issue. The review by Park et al. highlights that the reported prevalence of ED across Asian countries ranges widely—from as low as 2% to as high as 88%—depending on methodology, age structure, and assessment tools . Such variability does not diminish the central finding: ED is common, underreported, and insufficiently treated.
The modern era of ED management was transformed by the introduction of phosphodiesterase type-5 (PDE-5) inhibitors, beginning with sildenafil. These agents have demonstrated consistent efficacy across diverse Asian populations in randomized clinical trials . Yet pharmacology alone cannot resolve epidemiologic and cultural barriers. To understand ED in Asia is to understand not only vascular biology but also social silence, health system access, and the psychology of masculinity.
This article synthesizes epidemiological data, cultural influences, and therapeutic evidence—particularly regarding sildenafil and other PDE-5 inhibitors—while translating scientific findings into practical clinical insight.
Epidemiology of Erectile Dysfunction in Asia: Wide Numbers, Clear Message
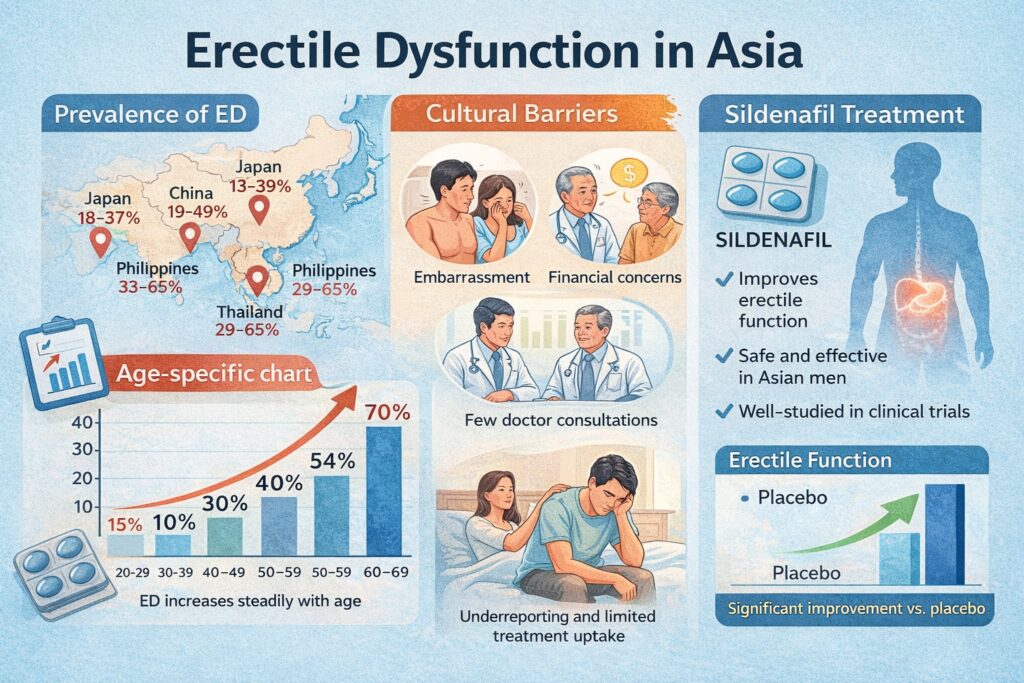
The prevalence of ED in Asia varies substantially between countries and studies. A meta-analysis cited in the review reported rates ranging from 2% to 81.8%, with age-standardized prevalence approaching 36.8% . When age stratification is applied, the trend becomes unmistakable: prevalence increases steadily with advancing age, exceeding 70% in men aged 60–69 in pooled analyses.
The heterogeneity stems from methodological differences. Some studies relied on self-reporting, others used validated instruments such as the International Index of Erectile Function (IIEF). Even among IIEF-based studies, validated translations were not always available in local languages . Thus, the epidemiological variation reflects measurement inconsistency as much as biological diversity.
Nevertheless, several large surveys converge on a consistent conclusion. The Global Study of Sexual Attitudes and Behaviors (GSSAB) subgroup analysis in Asian countries revealed ED prevalence rates of 33% in the Philippines, 29% in Thailand, 28% in Malaysia, 18% in Korea, and 13% in Japan . The Asian Survey of Aging Males reported ED in 63% of men aged 50–80 across five Asian regions . Even if one discounts methodological inflation, the burden remains substantial.
In short, ED in Asia is not rare—it is epidemiologically entrenched.
Age, Comorbidity, and the Vascular Axis
Age remains the strongest predictor of ED. As demonstrated in both Western and Asian cohorts, erectile function declines progressively with advancing years. However, age acts largely through vascular and metabolic intermediaries rather than as an isolated factor.
ED is strongly associated with diabetes mellitus, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease . These conditions converge on a shared pathophysiological pathway: endothelial dysfunction. The penile arteries, with a smaller diameter than coronary vessels, often manifest symptoms of vascular compromise earlier—a phenomenon sometimes referred to as the “artery size hypothesis.”
In Asian populations, the epidemiological transition toward urbanization and Westernized dietary patterns has accelerated metabolic syndrome prevalence. This shift inevitably influences ED rates. The interplay between diabetes and ED is particularly pronounced; hyperglycemia induces oxidative stress, nitric oxide depletion, and cavernosal smooth muscle dysfunction.
Thus, ED in Asia cannot be divorced from cardiovascular medicine. It is frequently the first visible manifestation of systemic endothelial pathology.
Cultural Attitudes and the Silence Surrounding Sexual Health
Perhaps the most striking aspect of ED in Asia is not its prevalence but its underreporting. The GSSAB study showed that most men and women with sexual dysfunction had not consulted a physician . Only a minority had ever been asked about sexual health during routine care.
Cultural influences play a decisive role. In East Asia, Confucian traditions emphasize modesty and restraint in discussing sexuality. In Southeast Asia, religious contexts—Buddhist, Muslim, or Catholic—shape attitudes differently but often maintain a degree of conservatism. In several countries, men preferred seeking advice from partners or family members rather than physicians .
Economic barriers further compound silence. Access to specialized urologic care varies significantly between regions, and medication costs may deter consultation . The paradox is evident: ED is common, effective treatments exist, yet many men do not seek help.
Public education campaigns and physician-initiated conversations remain critical. Without normalization of sexual health discourse, even the most effective pharmacotherapy will remain underutilized.
The Therapeutic Revolution: PDE-5 Inhibitors in Asian Populations
The advent of PDE-5 inhibitors fundamentally altered ED management. Five agents have been studied in Asian populations: sildenafil, vardenafil, tadalafil, udenafil, and mirodenafil . Across randomized controlled trials, these drugs consistently outperformed placebo in improving IIEF scores and sexual encounter success rates.
A systematic review encompassing 130 RCTs confirmed that oral PDE-5 inhibitors improve erectile function with comparable efficacy and safety profiles . Asian-specific trials mirrored Western data, dispelling concerns about ethnic pharmacodynamic differences.
Adverse events were typically mild—headache, flushing, dyspepsia, nasal congestion—and discontinuation rates were low . These safety findings are clinically important, particularly in populations where medication hesitancy may already be present.
Among these agents, sildenafil remains the most historically and clinically influential.
Sildenafil: Clinical Evidence in Asian Men
Sildenafil was the first PDE-5 inhibitor introduced and remains a benchmark for efficacy. The Asian Sildenafil Efficacy and Safety Study (ASSESS) series evaluated sildenafil in Malaysia, Singapore, the Philippines, Thailand, Taiwan, and Korea .
In ASSESS-1, ASSESS-2, and ASSESS-3, sildenafil significantly improved erectile function domain scores of the IIEF, as well as successful intercourse attempts, compared with placebo . Improvement in IIEF question 3 (penetration ability) and question 4 (maintenance of erection) was statistically robust, often with P values below 0.0001.
The Korean ASSESS-K trial confirmed similar findings over eight weeks . Importantly, efficacy was observed across diverse etiologies, including vascular and psychogenic components. Adverse effects—flushing, headache, mild visual disturbance—were generally transient.
From a mechanistic standpoint, sildenafil enhances nitric oxide–mediated vasodilation by inhibiting PDE-5–mediated degradation of cyclic guanosine monophosphate (cGMP). In practical terms, it restores the hemodynamic cascade necessary for erection in the presence of sexual stimulation.
Clinically, sildenafil’s flexibility in dosing (25–100 mg) and well-characterized safety profile make it an accessible first-line therapy throughout Asia.
Beyond Sildenafil: Regional Innovations
Two PDE-5 inhibitors—udenafil and mirodenafil—were developed and studied primarily in Korea . Udenafil offers a relatively rapid onset with prolonged duration of action, while mirodenafil demonstrates comparable selectivity and efficacy.
Randomized trials showed significant improvements in IIEF-EF scores and sexual encounter profiles with these agents compared to placebo . Adverse events were similar to those of sildenafil and tadalafil.
The emergence of regionally developed agents reflects both scientific capacity and market adaptation. However, clinical choice among PDE-5 inhibitors is often guided less by efficacy differences and more by pharmacokinetic preferences, patient tolerance, and cost considerations.
Clinical Implications: Integrating Epidemiology with Practice
The evidence suggests several clear clinical priorities:
- Routine inquiry about sexual health should be integrated into primary care visits.
- ED should be evaluated as a potential marker of cardiovascular disease.
- PDE-5 inhibitors, particularly sildenafil, should be offered as first-line therapy when not contraindicated.
- Sociocultural sensitivity must guide physician–patient communication.
Importantly, ED management in Asia must address both medical and psychological dimensions. A pill can restore vascular function, but it cannot alone dismantle stigma.
The Future of ED Management in Asia
Future research should focus on long-term outcomes in men with comorbidities such as diabetes and hypertension . There is also a need for harmonized epidemiological methodologies, including standardized IIEF translations and severity stratification.
Public health initiatives could transform ED care by normalizing discussion and reducing embarrassment. As cardiovascular screening improves, ED may increasingly serve as a sentinel symptom prompting early intervention.
Sildenafil and its pharmacological relatives have demonstrated their therapeutic value. The remaining challenge lies in ensuring equitable access and culturally competent care.
Conclusion
Erectile dysfunction in Asia is highly prevalent, frequently underreported, and consistently responsive to PDE-5 inhibitor therapy. Epidemiological data reveal wide numerical variation, yet the overall burden is unmistakable . Cultural conservatism and economic barriers hinder help-seeking behavior, even in the presence of effective treatment.
Randomized controlled trials confirm that sildenafil and other PDE-5 inhibitors significantly improve erectile function with acceptable safety profiles in Asian men . Sildenafil, in particular, remains a cornerstone of therapy, combining efficacy, flexibility, and extensive clinical validation.
The path forward requires integration of vascular medicine, sexual health education, and culturally aware communication. When these elements converge, ED becomes not a silent burden but a manageable condition with tangible solutions.
FAQ
1. How common is erectile dysfunction in Asia?
Reported prevalence ranges widely from 2% to 88%, depending on age and methodology, but overall data confirm that ED is common and increases with age .
2. Why do many Asian men not seek treatment?
Cultural conservatism, embarrassment, and financial barriers contribute to low consultation rates despite the availability of effective therapies .
3. Is sildenafil effective in Asian populations?
Yes. Multiple randomized controlled trials across Asian countries demonstrate significant improvements in erectile function compared with placebo .
4. Are PDE-5 inhibitors safe for long-term use?
They are generally well tolerated, with mostly mild adverse events. However, evaluation of cardiovascular status is essential before initiation.